






Imagine waiting years—sometimes decades—for a name to put to your suffering. That’s the reality for millions living with rare diseases. Over 7,000 known rare conditions exist, and roughly 80% have a genetic origin. Yet, diagnosis often feels like a lottery. Enter personalized medicine. It’s not just a buzzword; it’s a lifeline. Let’s explore how tailoring treatment to your DNA is rewriting the diagnostic playbook.
The Diagnostic Odyssey: Why Rare Diseases Are So Hard to Pin Down
Here’s the thing—rare diseases are, well, rare. Each one affects fewer than 200,000 people in the U.S. But collectively, they impact over 300 million globally. Symptoms often mimic common illnesses. A patient might see five, ten, even fifteen specialists before getting an answer. It’s exhausting. And expensive. The average rare disease patient spends four to five years searching for a diagnosis. That’s not just time lost; it’s hope deferred.
Traditional diagnostic tools—like standard blood tests or imaging—often miss the mark. Why? Because they’re designed for the “typical” patient. But rare disease patients? They’re anything but typical. That’s where personalized medicine steps in, shifting the focus from population averages to individual biology.
What Exactly Is Personalized Medicine? (And Why It’s a Game-Changer)
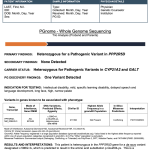
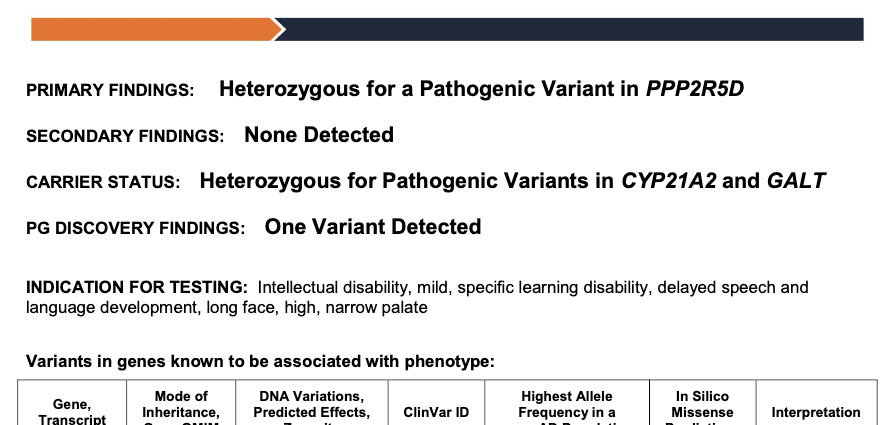
Honestly, personalized medicine sounds fancy, but it’s pretty straightforward. It’s about using your unique genetic, environmental, and lifestyle data to guide care. Think of it like a custom-tailored suit versus off-the-rack. For rare diseases, the key tool is genomic sequencing—reading your entire DNA code to spot the glitch causing the illness.
But it’s not just about genes. It’s about integrating that data with clinical history, family trees, and even wearable device metrics. The result? A diagnosis that’s yours, not a textbook definition. And for rare diseases, that’s revolutionary.
How Genomic Sequencing Is Shortening the Diagnostic Odyssey
Let’s get into the nitty-gritty. Whole exome sequencing (WES) and whole genome sequencing (WGS) are the heavy hitters here. WES looks at the protein-coding parts of your DNA—about 1-2% of the genome. WGS reads the entire thing. Sounds like overkill? Not for rare diseases. Many mutations hide in non-coding regions, which WGS catches.
A study in Genetics in Medicine found that WGS increased diagnostic yield by 34% compared to standard testing. That’s huge. For a family who’s been searching for years, a 34% better chance is everything. I’ve heard stories of kids finally getting a name for their condition after a decade—thanks to a single sequencing test.
Real-World Example: The Undiagnosed Diseases Network
The Undiagnosed Diseases Network (UDN) is a perfect case. They use personalized approaches—including WGS and RNA sequencing—to crack the toughest cases. In one instance, a child with mysterious seizures was found to have a mutation in a gene linked to potassium channels. That discovery? It led to a targeted treatment that stopped the seizures. No more guessing. No more trial-and-error.
Beyond Sequencing: The Role of Big Data and AI
Sequencing is step one. But you know what happens next? You get a mountain of data. Like, 100 gigabytes per genome. That’s where AI and machine learning come in. Algorithms can sift through millions of variants, comparing them to global databases to find the needle in the haystack. It’s like having a super-sleuth detective who never sleeps.
Some platforms—like Phenotips or Face2Gene—even use facial recognition software. They analyze subtle facial features that might point to a specific syndrome. Sounds sci-fi, right? But it’s real. And it’s helping doctors narrow down possibilities in minutes, not months.
Challenges: It’s Not All Smooth Sailing
Look, I’d love to say personalized medicine is a magic bullet. But it’s not—at least not yet. Here are some hurdles:
- Cost: Whole genome sequencing can run $1,000 to $5,000. Insurance coverage is spotty. For many families, that’s a huge barrier.
- Data interpretation: We find a lot of “variants of uncertain significance.” Basically, we see a change in the DNA but don’t know if it’s harmful. That can lead to more anxiety, not less.
- Access: Not every hospital has a genetic counselor or a bioinformatics team. Rural areas? Forget it. The gap between urban and rural access is stark.
- Ethical concerns: Who owns your genomic data? Could it be used against you by insurers or employers? The GINA Act offers some protection, but it’s not perfect.
Still, these challenges are being tackled. Costs are dropping. AI is getting smarter. And advocacy groups are pushing for broader insurance coverage. Progress, you know, is rarely linear.
Personalized Medicine in Action: A Quick Look at Key Tools
Let’s break down some of the most impactful tools right now. I’ve thrown them into a table for clarity—because sometimes a table just makes sense.
| Tool | What It Does | Impact on Rare Disease Diagnosis |
|---|---|---|
| Whole Genome Sequencing | Reads all 3 billion base pairs of your DNA | Catches hidden mutations in non-coding regions |
| RNA Sequencing | Measures gene expression levels | Reveals if a mutation actually affects protein production |
| Exosome Analysis | Looks at tiny vesicles shed by cells | Can detect disease markers before symptoms appear |
| AI Phenotyping | Matches patient symptoms to known syndromes | Reduces diagnostic time from years to weeks |
| CRISPR-based Diagnostics | Uses gene-editing tech to spot mutations | Portable, cheap, and fast—ideal for field use |
Notice how each tool builds on the other? That’s the beauty of a personalized approach. It’s not one-size-fits-all. It’s a toolkit you mix and match based on the patient.
The Human Side: Stories That Stick
I remember reading about a woman named Sarah. She’d been sick for 15 years—chronic pain, fatigue, weird rashes. Doctors called it fibromyalgia, lupus, even “stress.” Finally, a research clinic offered her whole genome sequencing. Turned out she had a rare mitochondrial disorder. The treatment? High-dose vitamins and a specific diet. Within months, she felt like a new person. Not cured, but understood. That’s the power of a name.
Stories like Sarah’s aren’t rare—they’re the norm in this field. Personalized medicine doesn’t just diagnose; it validates. It says, “You’re not crazy. Your suffering is real. And here’s why.”
What’s Next? The Future of Rare Disease Diagnosis
We’re moving toward a world where every newborn gets a genome sequenced at birth. That’s already happening in pilot programs—like the BabySeq project. Imagine catching a rare disease before symptoms even appear. Prevention, not just reaction. That’s the dream.
Also, watch for liquid biopsies. These blood tests can detect tumor DNA or fetal DNA in pregnancy, but they’re being adapted for rare genetic conditions. Non-invasive, quick, and surprisingly accurate. And then there’s the rise of patient-driven registries—platforms where rare disease patients share their data to accelerate research. It’s a community effort, really.
Final Thoughts: A Diagnosis Is Just the Beginning
Personalized medicine isn’t a cure-all. It’s a tool—a powerful one. It shortens the diagnostic odyssey, reduces guesswork, and gives families a roadmap. But it also raises questions we’re still grappling with: equity, privacy, and the sheer complexity of human biology. Yet, for the millions wandering in diagnostic limbo, it’s a beacon. A name for the pain. A path forward.
And honestly? That’s worth fighting for.